Abilities In Motion is always seeking new and innovative ways to meet the needs of our patients… including athletes. www.abilitiesinmotion.com
Before losing his leg in a vehicle accident, Scott Lane ran marathons. Abilities In Motion working to equip him for his next race and his active lifestyle.
“We’ve seen Scott over the years, so we know what works for him. We give him the latest running feet to trial and he picks the one that he likes.”
Scott’s prosthesis was fit with a custom cover printed in our lab on our 3D printer. Innovation is a core value at Abilities In Motion as we continue equiping athletes with cutting edge prosthetic legs.
Scott Lane’s Endolite Echelon foot with custom cover.
We have two locations. Our main office is a state-of-the-art facility at 11151 Kenwood Road, Cincinnati, Ohio. Our second facility, which is located at 5701 Cheviot Road in Cincinnati, Ohio, was opened by Thomas L. Walsh, CPO, LPO, FAAOP in August of 1995 to serve the greater Cincinnati, southeastern Indiana, and northern Kentucky areas.
We would love to hear from you. Just give us a call at (513) 245-0253.
Abilities In Motion is an ABC accredited Prosthetic facility.
Abilities In Motion proudly announces a Three-Year Accreditation award in orthotics and prosthetics by the American Board for Certification in Orthotics, Prosthetics & Pedorthics, Inc. (ABC).
Abilities In Motion is recognized for achievements in the areas of Organizational Management, Patient Care Standards, Quality Assurance, Supplier Compliance and Facility and Safety Management. This award represents the highest level of accreditation achievable in the profession of orthotics and prosthetics.
“It’s great to be recognized by ABC as they are the standard bearer for our industry,” said Matthew Milthaler, a member of the Abilities In Motion Team. “This accreditation simply acknowledges the commitment our team has to provide outstanding care for our patients.”
“Abilities In Motion has demonstrated its commitment to the provision of quality patient care services by seeking and attaining ABC accreditation,” said Catherine Carter, ABC’s Executive Director. “ABC has developed the highest standards for accreditation in the industry and is proud to include Abilities In Motion among our over 2500 accredited patient care facilities.”
The American Board for Certification in Orthotics, Prosthetics and Pedorthics, Inc. has been credentialing practitioners and organizations since 1948 in accordance with established standards of excellence in the delivery of comprehensive patient care. A not-for-profit organization headquartered in Alexandria, Virginia, ABC’s mission is to encourage and promote the highest standards of professionalism in the delivery of orthotic, prosthetic and pedorthic services. ABC advances the competency of practitioners, promotes the quality and effectiveness of orthotic, prosthetic, and pedorthic care, and maintains the integrity of the profession.
“It’s great to be recognized by ABC as they are the standard bearer for our industry,” said Matthew Milthaler, a member of the Abilities In Motion Team. “This accreditation simply acknowledges the commitment our team has to provide outstanding care for our patients.”
Completed removable immediate postoperative cast with Velcro straps attached to base plates.
Abilities In Motion has been leading the way with Immediate Postoperative Prosthesis (IPOP) procedures since 1995. This course of treatment has become preferred by doctors for individuals facing below the knee amputation. After the surgeon has completed their work, our staff creates a removable cast that protects the incision site, reduces swelling, decreases pain and allows the physicians to conduct regular inspections of the residual limb. In some cases, a temporary prosthesis can be attached to make it possible for some patients walk weeks after surgery.
Led by Tom Walsh, Abilities In Motion is always seeking new and innovative ways to meet the needs of our patients. Tom was a pioneer in designing a removable immediate post operative cast or prosthesis. This unique, previously unavailable service helps patients, surgeons and physical therapists obtain better outcomes.
Below are some quick facts about the procedure followed by an academic article that was published in the Journal of Prosthetics and Orthotics by Abilities In Motion’s own Tom Walsh. If you have any questions, please contact us live chat (below), by phone: (513) 245-0253 or by email.
Purpose
Immobilizes wound to improve healing
Controls edema
Avoids knee flexion contracture
Protects the incision from extrinsic trauma
Removable for wound inspection
Improved Healing Rate
Studies report that with the use of immediate post operative prosthesis and amputation level selection by xenon clearance, healing approached 100%.
Prior to the use of immediate post operative prosthesis, the primary healing rate ranged from 62% to 75%.
History of Immediate Post Operative Prosthesis
IPOP procedure originated in the late 1950’s.
Studies report with use of IPOP, prosthetic rehabilitation improved from 64% to 100% for unilateral amputees who had been ambulatory before amputation*.
Initially the IPOP was not easily removable, but in 1995 at surgeons requests, Tom Walsh, CPO, LPO, FAAOP designed the removable IPOP.
Many postoperative treatment modalities for the transtibial amputee are in current use. A simple gauze dressing is the treatment of choice for many surgeons. Another option is compression therapy using an ace bandage or stump shrinker. A more aggressive approach would include the use of a rigid dressing or an immediate postoperative prosthesis (IPOP).
Figure 1. Three spandex socks, suprapatellar gel pad, distal tibia and suture line gel pad, foam distal end pad, and attachment plate.
The latter modality, although documented to offer the highest rate of healing, is possibly the least used because of many factors, including lack of familiarity with the treatment, a fear of placing a hard cast on a vascularly compromised limb, and the need to frequently monitor the wound. The traditional IPOP is a nonremovable cylinder cast. When the residual limb needs to be inspected, the cast is cut off using a cast saw. Another cast is then fabricated if the IPOP continues to be used. This article presents a removable IPOP, designed for the diabetic, peripheral vascular disease amputee, that specifically addresses the needs of the surgeon. In addition, the design permits a proactive clinical team approach, enhancing the treatment of the prosthetist and the physical therapist. (J Prosthet Orthot. 2003;15:158–161.)
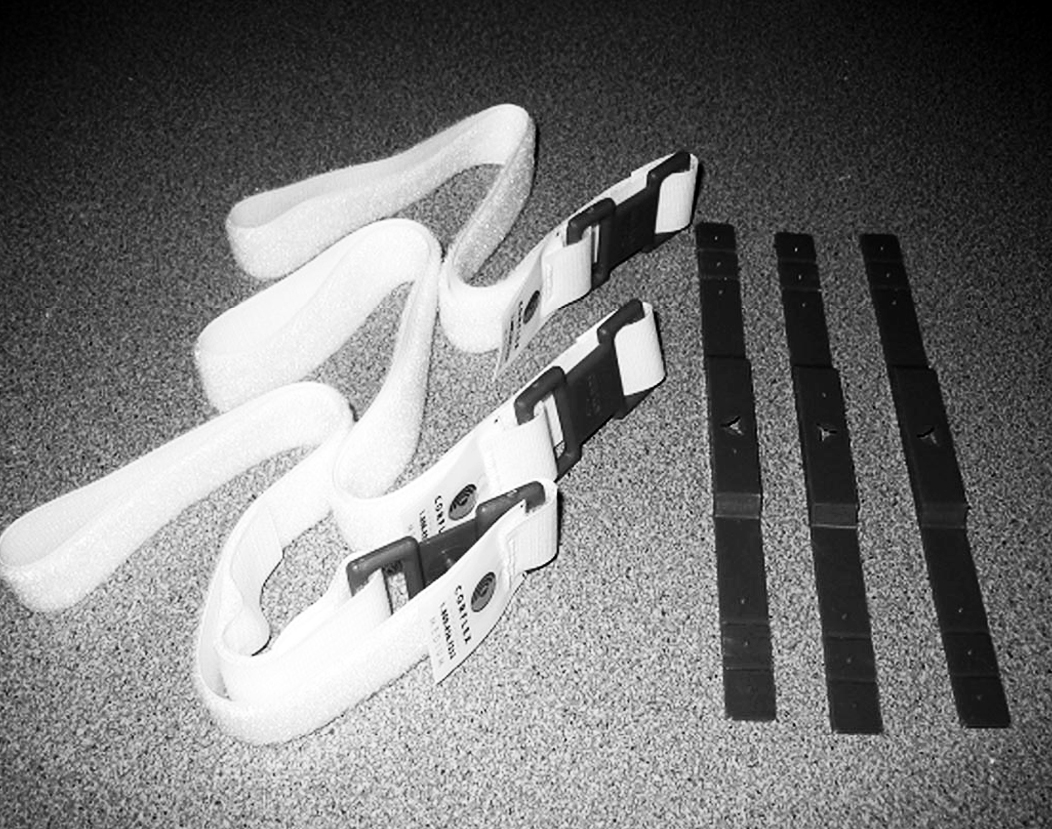
Figure 2. Three strap attachment base plates, three Velcro straps.
The concept of immediate postoperative prosthetic fittings (IPPF) is not new. In 1893, German surgeon von Bier reported fitting patients with temporary prostheses within days of amputation and allowed them to stand and walk. In 1961, Berlemont reported fitting patients with prostheses immediately after amputation surgery and initiating gait training in 1 to 2 days. In 1971, Burgess reported satisfactory results in 193 lower extremity amputations performed for peripheral arterial insufficiency; by 1978, he and his group had performed more than 1500 consecutive unselected amputations with the IPPF approach. Moore5 reports a considerable range of healing rates in literature before the use of immediate postoperative prosthesis (IPOP). The primary healing rate ranged from 62 to 75%. With the use of IPOP and amputation level selection by xenon clearance, healing approached 100%. In addition, Moore reports improved rehabilitation rates. Before the use of IPOP, the average rate of prosthetic rehabilitation in the geriatric amputee was 64%. With the use of the IPOP, a 100% prosthetic rehabilitation rate was achieved in unilateral amputees who had been ambulatory before amputation. More recently, in 1987, Wu and Krick reported the use and success of a removable rigid dressing. Although the primary purpose of their design was a non–weight-bearing rigid dressing, many of the principles are the same.
Despite these reported successes, use of the IPOP is not the standard of treatment for postoperative management of the amputee in the 21st century. Surgeons often cite the concern of skin breakdown and the need to inspect the surgical site for proper healing. The patient often lacks sensation and is unable to detect or report excessive pressure or friction caused by the cast. Often, the amputee is a geriatric patient with poor strength, and the potential for rehabilitation is unknown.
Still the overall purpose and results of the IPOP cannot be ignored. An IPOP may:
Assist in wound healing and residual limb maturation
Minimize postsurgical edema and pain
Provide psychological benefit of early ambulation
Reduce phantom pain and the effects of inactivity through controlled weight bearing and ambulation
Control or prevent knee flexion contracture
Protect the residual limb from trauma, such as a fall
The purpose of this article is to present an easily and quickly fabricated IPOP designed to allow removal for wound inspection. By being removable, the design not only meets the needs of the surgeon but also benefits the entire rehabil- itation process. The prosthetist is allowed to make adjust- ments to accommodate for volume changes and to aid in limb shaping. The physical therapist is allowed to perform strengthening and range of motion exercises to the knee. The result is faster healing and a greater chance for successful rehabilitation.
APPLICATION
Upon completion of the amputation, the surgeon applies a dressing of choice. It is important to note that the thickness of the dressing must be maintained throughout the process. Typically, the dressing does not extend proximal to the knee.
Figures 1 and 2 show the items needed in preparation for casting.
Figure 1. Three spandex socks, suprapatellar gel pad, distal tibia and suture line gel pad, foam distal end pad, and attachment plate.Three strap attachment base plates, three Velcro straps.
Two spandex socks are applied over the dressing.
A gel pad is placed over the patella and extends proximal to the patella by 1 inch.
A distal foam pad is applied, followed by a second gel pad that covers the suture line and distal, anterior aspect of the tibia.
A third spandex sock is applied.
Fiberglass casting tape (5-inch width) is applied to the distal aspect of the limb extending proximal to the knee joint.
A prosthetic attachment plate is wrapped into the cast and set in proper alignment.
The cast is then extended proximally to 2–4 inches
below the perineum. As the cast sets, pressure is applied with the flat of the hand on the medial and lateral sides of the thigh just proximal to the knee to assist with suspension and rotation control. No pressure is applied or cast shaping done distal to the knee to insure total contact pressure.
Typically, on postoperative day 1, the cast is bivalved and Velcro straps are applied.
Cut lines are marked along with placement of strap anchors. The anterior cut line should be approximately 2 inches proximal to the prosthetic attachment plate. This allows for easy removal and reapplication of the cast. A strap anchor is placed on the posterior lateral shell just proximal to the anterior distal cut line. A second strap anchor is placed on the anterior shell just proximal and lateral to the patella. The third strap anchor is placed most proximal on the anterior shell. (Figure 3)
Figure 3. Fiberglass immediate postoperative cast with bivalve cut lines and base plate attachment points. Note the triangle index cuts on the medial and lateral sides of the cast that key the anterior and posterior sections together.
The cast is moistened with water. Water helps the second layer of casting tape adhere to the first. The strap anchors are wrapped into the cast with a single layer of casting tape.
As the cast sets, attachment points on the anchors for the straps are exposed using a knife.
The cast is bivalved along the cut lines. The cast is separated and the outer spandex sock is cut. (Figure 4)
Figure 4. Bivalved cast with base plates wrapped into the cast.
A window relief is cut out for the patella. The gel pad is modified to fit in the cast superior to the patella and adhered to the cast using double-sided tape. Proximal to the patella can be an area of high pressure (Figure 5).
Figure 5. Anterior and posterior sections of cast. Note the placement of the gel pads superior to the patella cut out and along the suture line covering the distal tibia.
The gel pad covering the suture line and distal tibia is cut along the bivalve cut line and adhered to the inside of the cast using double-sided tape (Figure 5).
The distal foam pad is cut accordingly along the bivalve cut line (medial and lateral only; anterior is not cut).
Velcro straps are mounted to the base plates and fastened (Figure 6).
Figure 6. Completed removable immediate postoperative cast with Velcro straps attached to base plates.
POSTOPERATIVE REGIMEN
A physical therapy evaluation is ordered and rehabilitation goals are set. Usually, standing and transfers are the initial goals, followed by hopping with a walker. If the patient is able to hop with the use of a walker or parallel bars, then the use of the pylon and prosthetic foot can be considered. The pylon and foot are attached, and 20 – 40 pounds of weight bearing is permitted. Zettl7 recommends 20 pounds of weight bearing and states that full weight bearing or weight bearing to tolerance can be counter-productive. A 20-pound weight- bearing limit has been found to be difficult to maintain during walking; therefore, the weight-bearing limit of 40 pounds has been permitted with good results. Typically, a scale is placed under the prosthetic foot and the patient is allowed to shift weight onto the IPOP and receive visual feedback as to when the weight bearing limit is achieved. The patient is then instructed to raise the contralateral limb while still maintaining the 20–40 pounds of weight bearing. When these goals are achieved, walking can begin (Figure 7),
Figure 7. Ambulating with the removable IPOP limiting weight bearing to 20 – 40 pounds.
In- struction on stairs and ramps follows. The pylon and foot are removed at the end of the physical therapy session. Once all goals are met, the amputee may use the pylon and foot for all activities of daily living. The patient is instructed on the application and removal of the pylon and foot, which can be
removed for sleeping or for activities such as getting into a vehicle. If the pylon and foot are worn during sitting for long periods, it is recommended that a footrest be used for sup- port.
Strengthening and range-of-motion exercises may be per- formed by removing the IPOP cast for short periods (Figure 8). The residual limb may have a tendency to swell when out of the cast and therefore should not be left out of the cast for more than 5–10 minutes. These exercises usually begin after the first wound inspection.
Figure 8. Immediate postoperative cast removed to allow physical therapy strengthening and range of motion exercises.
Postoperative management of the amputee should include measures to prevent falls. Barr et al. found that patients who have a primary diagnosis of lower limb amputation were five times more likely to fall than those who had a different primary diagnosis. A fall for the amputee can result in wound separation, often needing revision surgery. The IPOP provides a padded protective environment for wound healing. With the pylon and foot in place, the amputee functions with a more stable, bipedal gait.
For the surgeon to inspect the wound, the prosthetist does not have to be present. The surgeon simply unfastens the Velcro straps and removes the anterior shell of the cast. Instructing the patient to raise the extremity off of the bed by flexing at the hip, the posterior half of the cast can be removed. The Spandex cast socks are removed followed by the dressing. Make note that when reapplying the IPOP cast, the thickness of the gauze dressing must be maintained. The tendency is to apply a lighter dressing, which is counter-productive to maintaining distal compression. The fit of the IPOP cast must be continually monitored. By approximately postoperative day, the residual limb may experience a loss of edema and the IPOP cast becomes loose. An additional Spandex cast sock is applied to improve the fit of the cast and promote further shrinkage of the residual limb. Cast socks continue to be added throughout the time the cast is in place. A sock covering only the distal end of the limb is often used when distal shrinkage is not consistent with the thigh.
On the average, sutures are removed 21–28 days postop- eratively. After suture removal, a total contact below-the- knee prosthesis is fabricated to allow full weight bearing. If possible, the IPOP continues to be used until the total contact below the knee prosthesis is fitted, thereby maintaining func- tion and protection.
CONCLUSION
For the past 7 years, the removable IPOP has proven to be an effective adaptation to the original IPOP concept. The initial goal of the design was to meet the needs of the surgeon, which was to allow for easy wound inspection. The design later proved to be beneficial in the area of physical therapy to allow for strengthening and range of motion. In addition, the prosthetist is aided by the ability to adjust for residual limb volume loss and assist in limb shaping. All lead to a more cohesive clinical team approach with a better understanding of the challenges of postoperative management.
1. Dederich R. Amputationen der unteren Extremitat. Operation- stechnik und prothetische Sofortversorgung. Stuttgart, Thieme, 1970.
2. Berlemont M. Notre experience de l’appareillage precoce des amputes des membres inferieurs aux establissments Helio- Marins de Berck. Ann Med Phys. 1961;4:4.
3. Berlemont M, Weber R, Willot JP. Ten years of experience with immediate application of prosthetic devices to amputees of the lower extremities on the operating table. Prosthet Orthot Int. 1969;3:8.
4. Burgess EM. Immediate postsurgical prosthetic fitting: A system of amputee management. Am J Phys Ther. 1971;51:139–143.
5. Moore WS. Below-knee amputation. In: Moore WS, Malone JM, eds. Lower Extremity Amputation. Philadelphia: WB Saunders Company; 1989:118–131.
6. Wu Y, Krick H. Removable Rigid Dressing for Below-knee Am- putees. Clin Prosthet Orthot. 1987;11:33–44.
The Physical Therapy Assistant program at the University of Cincinnati, Clermont gained valuable, hands on experience today at Premiere Physical Therapy and Abilities in Motion.
Carolyn Shisler, who leads the program at UC, Clermont said that this experience gives future physical therapist assistants the opportunity to hear stories and ask questions to recent and veteran amputees. “They are real people and students are able to hear their story and empathize with their life situation. Our students get to see the person and not the diagnosis,” said Shisler.
Caitlin Rausch participates with PT Training
Caitlin Rausch is a student at UC, Claremont and she echoed those feelings. “It’s so different than being in the classroom. There, you don’t get to see patients and hear their backgrounds”.
Students heard an hour long presentation from experts and then broke into smaller groups to see demonstrations and interact with patients. The patients participating in the program had below knee, above knee and bilateral leg amputations. Each had different experiences that informed students and each saw this as an opportunity to invest in the future.
Andy Beardslee is the PT director at Premiere Physical Therapy and he understands the value of these types of experiences. “Many times, new students are apprehensive when meeting with amputees. They may have a fear of saying the wrong thing and this experience gives them a change to get comfortable with real people.”
Jay Estoquia is a resident at Abilities In Motion
Students would be hard pressed to find a better environment for this type of learning as Premier Physical Therapy is the regions leader in working with amputee patients. Their partnership with Abilities In Motion allows a patient to meet with their prosthetist and physical therapist all in same visit.
Shisler summed up the experience this way, “PTAs work in many different areas of physical therapy, Amputees are one facet of the field. It’s important that they are able to work with people and help them reach their full potential.”