Brian Donnellan has always been active, but two years ago he was hit with the news that his leg would need to be amputated below the knee. Over the past two years he has been partnering with Abilities In Motion to achieve his goals of an active lifestyle.
This past month, Brian took a two week European trip with stops in Ireland and Italy. “This was the best trip ever, because I got to do everything that I wanted to do,” said Brian. He also shared some pro tips with us about traveling with a prosthesis:
GET A TUNE UP. A few weeks before traveling, Brian made an appointment to see the experts at Abilities In Motion. They were able to check his prosthesis and were able to make adjustments before he traveled. Brian was also fitted with a swim leg*, which is a secondary device that is waterproof. This helped Brian use smaller showers that are typical when traveling internationally.
GIVE YOURSELF EXTRA TIME AT TSA. We have all been told to arrive early and allow extra time to get through security, but this is especially true when wearing a medical device. Brian strongly recommends using the handicap line when going through TSA. Brian also chose to wear shorts to make inspecting his leg easier.
CHECK AN EXTRA BAG. According to Air Carrier Access Act (ACAA), a suitcase that contains only “assistive devices” are exempt from checked bag fees. You will want to notify the agent that your bag contains such equipment and will likely be asked to open the bag to verify its contents. Remember, baggage can be misrouted or lost during travel, so it is important to make sure you carry on your most important equipment and supplies.
ASK FOR EXTRA LEG ROOM. Brian asked his airline for extra leg room to help accommodate his prosthesis. The airline responded to his request, and because he was comfortable assisting in the event of an emergency, this allowed him to sit in an exit row. During a longer flight, this extra room can be invaluable.
During his trip, Brian was able to enjoy the Cliffs of Moher. “I felt comfortable the entire time. My wife was a little concerned that I was standing on a 1,000 foot cliff, but it was easy,” says Brian. He was also able to walk though the Coliseum in Rome and walked for miles on his trip.
“I just proved to myself that I can do whatever I want to do, and nothing is holding me back now.”
HEAR THE INTERVIEW HERE:
Please note, the information contained in this post is based on this individual’s experience. Individual situations vary. We recommend that you do your own research to fully comply with TSA and airline policies and restrictions.
*Swim Leg: Standard prosthetic legs are not able to be exposed to water because of some components are not waterproof. Swim legs are designed for swimming, bathing and other aquatic activities. They are typically not covered by insurance, but Abilities In Motion works to help accommodate patients with affordable solutions when necessary.
Completed removable immediate postoperative cast with Velcro straps attached to base plates.
Abilities In Motion has been leading the way with Immediate Postoperative Prosthesis (IPOP) procedures since 1995. This course of treatment has become preferred by doctors for individuals facing below the knee amputation. After the surgeon has completed their work, our staff creates a removable cast that protects the incision site, reduces swelling, decreases pain and allows the physicians to conduct regular inspections of the residual limb. In some cases, a temporary prosthesis can be attached to make it possible for some patients walk weeks after surgery.
Led by Tom Walsh, Abilities In Motion is always seeking new and innovative ways to meet the needs of our patients. Tom was a pioneer in designing a removable immediate post operative cast or prosthesis. This unique, previously unavailable service helps patients, surgeons and physical therapists obtain better outcomes.
Below are some quick facts about the procedure followed by an academic article that was published in the Journal of Prosthetics and Orthotics by Abilities In Motion’s own Tom Walsh. If you have any questions, please contact us live chat (below), by phone: (513) 245-0253 or by email.
Purpose
Immobilizes wound to improve healing
Controls edema
Avoids knee flexion contracture
Protects the incision from extrinsic trauma
Removable for wound inspection
Improved Healing Rate
Studies report that with the use of immediate post operative prosthesis and amputation level selection by xenon clearance, healing approached 100%.
Prior to the use of immediate post operative prosthesis, the primary healing rate ranged from 62% to 75%.
History of Immediate Post Operative Prosthesis
IPOP procedure originated in the late 1950’s.
Studies report with use of IPOP, prosthetic rehabilitation improved from 64% to 100% for unilateral amputees who had been ambulatory before amputation*.
Initially the IPOP was not easily removable, but in 1995 at surgeons requests, Tom Walsh, CPO, LPO, FAAOP designed the removable IPOP.
Many postoperative treatment modalities for the transtibial amputee are in current use. A simple gauze dressing is the treatment of choice for many surgeons. Another option is compression therapy using an ace bandage or stump shrinker. A more aggressive approach would include the use of a rigid dressing or an immediate postoperative prosthesis (IPOP).
Figure 1. Three spandex socks, suprapatellar gel pad, distal tibia and suture line gel pad, foam distal end pad, and attachment plate.
The latter modality, although documented to offer the highest rate of healing, is possibly the least used because of many factors, including lack of familiarity with the treatment, a fear of placing a hard cast on a vascularly compromised limb, and the need to frequently monitor the wound. The traditional IPOP is a nonremovable cylinder cast. When the residual limb needs to be inspected, the cast is cut off using a cast saw. Another cast is then fabricated if the IPOP continues to be used. This article presents a removable IPOP, designed for the diabetic, peripheral vascular disease amputee, that specifically addresses the needs of the surgeon. In addition, the design permits a proactive clinical team approach, enhancing the treatment of the prosthetist and the physical therapist. (J Prosthet Orthot. 2003;15:158–161.)
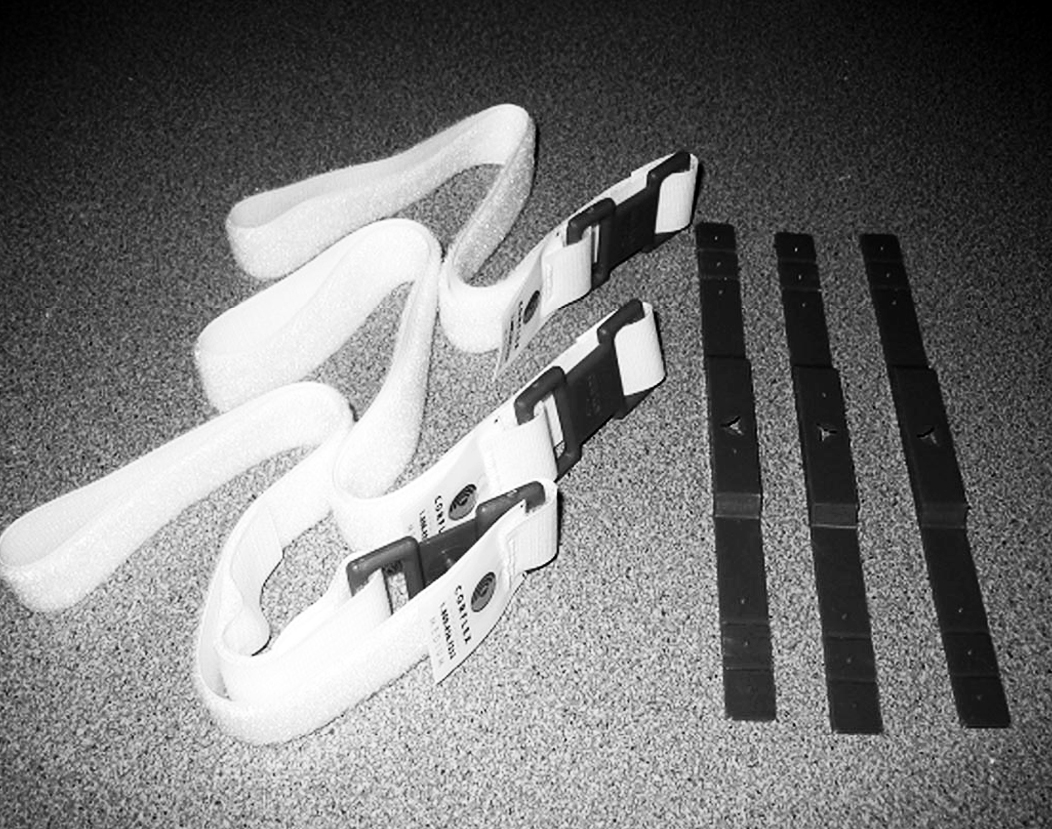
Figure 2. Three strap attachment base plates, three Velcro straps.
The concept of immediate postoperative prosthetic fittings (IPPF) is not new. In 1893, German surgeon von Bier reported fitting patients with temporary prostheses within days of amputation and allowed them to stand and walk. In 1961, Berlemont reported fitting patients with prostheses immediately after amputation surgery and initiating gait training in 1 to 2 days. In 1971, Burgess reported satisfactory results in 193 lower extremity amputations performed for peripheral arterial insufficiency; by 1978, he and his group had performed more than 1500 consecutive unselected amputations with the IPPF approach. Moore5 reports a considerable range of healing rates in literature before the use of immediate postoperative prosthesis (IPOP). The primary healing rate ranged from 62 to 75%. With the use of IPOP and amputation level selection by xenon clearance, healing approached 100%. In addition, Moore reports improved rehabilitation rates. Before the use of IPOP, the average rate of prosthetic rehabilitation in the geriatric amputee was 64%. With the use of the IPOP, a 100% prosthetic rehabilitation rate was achieved in unilateral amputees who had been ambulatory before amputation. More recently, in 1987, Wu and Krick reported the use and success of a removable rigid dressing. Although the primary purpose of their design was a non–weight-bearing rigid dressing, many of the principles are the same.
Despite these reported successes, use of the IPOP is not the standard of treatment for postoperative management of the amputee in the 21st century. Surgeons often cite the concern of skin breakdown and the need to inspect the surgical site for proper healing. The patient often lacks sensation and is unable to detect or report excessive pressure or friction caused by the cast. Often, the amputee is a geriatric patient with poor strength, and the potential for rehabilitation is unknown.
Still the overall purpose and results of the IPOP cannot be ignored. An IPOP may:
Assist in wound healing and residual limb maturation
Minimize postsurgical edema and pain
Provide psychological benefit of early ambulation
Reduce phantom pain and the effects of inactivity through controlled weight bearing and ambulation
Control or prevent knee flexion contracture
Protect the residual limb from trauma, such as a fall
The purpose of this article is to present an easily and quickly fabricated IPOP designed to allow removal for wound inspection. By being removable, the design not only meets the needs of the surgeon but also benefits the entire rehabil- itation process. The prosthetist is allowed to make adjust- ments to accommodate for volume changes and to aid in limb shaping. The physical therapist is allowed to perform strengthening and range of motion exercises to the knee. The result is faster healing and a greater chance for successful rehabilitation.
APPLICATION
Upon completion of the amputation, the surgeon applies a dressing of choice. It is important to note that the thickness of the dressing must be maintained throughout the process. Typically, the dressing does not extend proximal to the knee.
Figures 1 and 2 show the items needed in preparation for casting.
Figure 1. Three spandex socks, suprapatellar gel pad, distal tibia and suture line gel pad, foam distal end pad, and attachment plate.Three strap attachment base plates, three Velcro straps.
Two spandex socks are applied over the dressing.
A gel pad is placed over the patella and extends proximal to the patella by 1 inch.
A distal foam pad is applied, followed by a second gel pad that covers the suture line and distal, anterior aspect of the tibia.
A third spandex sock is applied.
Fiberglass casting tape (5-inch width) is applied to the distal aspect of the limb extending proximal to the knee joint.
A prosthetic attachment plate is wrapped into the cast and set in proper alignment.
The cast is then extended proximally to 2–4 inches
below the perineum. As the cast sets, pressure is applied with the flat of the hand on the medial and lateral sides of the thigh just proximal to the knee to assist with suspension and rotation control. No pressure is applied or cast shaping done distal to the knee to insure total contact pressure.
Typically, on postoperative day 1, the cast is bivalved and Velcro straps are applied.
Cut lines are marked along with placement of strap anchors. The anterior cut line should be approximately 2 inches proximal to the prosthetic attachment plate. This allows for easy removal and reapplication of the cast. A strap anchor is placed on the posterior lateral shell just proximal to the anterior distal cut line. A second strap anchor is placed on the anterior shell just proximal and lateral to the patella. The third strap anchor is placed most proximal on the anterior shell. (Figure 3)
Figure 3. Fiberglass immediate postoperative cast with bivalve cut lines and base plate attachment points. Note the triangle index cuts on the medial and lateral sides of the cast that key the anterior and posterior sections together.
The cast is moistened with water. Water helps the second layer of casting tape adhere to the first. The strap anchors are wrapped into the cast with a single layer of casting tape.
As the cast sets, attachment points on the anchors for the straps are exposed using a knife.
The cast is bivalved along the cut lines. The cast is separated and the outer spandex sock is cut. (Figure 4)
Figure 4. Bivalved cast with base plates wrapped into the cast.
A window relief is cut out for the patella. The gel pad is modified to fit in the cast superior to the patella and adhered to the cast using double-sided tape. Proximal to the patella can be an area of high pressure (Figure 5).
Figure 5. Anterior and posterior sections of cast. Note the placement of the gel pads superior to the patella cut out and along the suture line covering the distal tibia.
The gel pad covering the suture line and distal tibia is cut along the bivalve cut line and adhered to the inside of the cast using double-sided tape (Figure 5).
The distal foam pad is cut accordingly along the bivalve cut line (medial and lateral only; anterior is not cut).
Velcro straps are mounted to the base plates and fastened (Figure 6).
Figure 6. Completed removable immediate postoperative cast with Velcro straps attached to base plates.
POSTOPERATIVE REGIMEN
A physical therapy evaluation is ordered and rehabilitation goals are set. Usually, standing and transfers are the initial goals, followed by hopping with a walker. If the patient is able to hop with the use of a walker or parallel bars, then the use of the pylon and prosthetic foot can be considered. The pylon and foot are attached, and 20 – 40 pounds of weight bearing is permitted. Zettl7 recommends 20 pounds of weight bearing and states that full weight bearing or weight bearing to tolerance can be counter-productive. A 20-pound weight- bearing limit has been found to be difficult to maintain during walking; therefore, the weight-bearing limit of 40 pounds has been permitted with good results. Typically, a scale is placed under the prosthetic foot and the patient is allowed to shift weight onto the IPOP and receive visual feedback as to when the weight bearing limit is achieved. The patient is then instructed to raise the contralateral limb while still maintaining the 20–40 pounds of weight bearing. When these goals are achieved, walking can begin (Figure 7),
Figure 7. Ambulating with the removable IPOP limiting weight bearing to 20 – 40 pounds.
In- struction on stairs and ramps follows. The pylon and foot are removed at the end of the physical therapy session. Once all goals are met, the amputee may use the pylon and foot for all activities of daily living. The patient is instructed on the application and removal of the pylon and foot, which can be
removed for sleeping or for activities such as getting into a vehicle. If the pylon and foot are worn during sitting for long periods, it is recommended that a footrest be used for sup- port.
Strengthening and range-of-motion exercises may be per- formed by removing the IPOP cast for short periods (Figure 8). The residual limb may have a tendency to swell when out of the cast and therefore should not be left out of the cast for more than 5–10 minutes. These exercises usually begin after the first wound inspection.
Figure 8. Immediate postoperative cast removed to allow physical therapy strengthening and range of motion exercises.
Postoperative management of the amputee should include measures to prevent falls. Barr et al. found that patients who have a primary diagnosis of lower limb amputation were five times more likely to fall than those who had a different primary diagnosis. A fall for the amputee can result in wound separation, often needing revision surgery. The IPOP provides a padded protective environment for wound healing. With the pylon and foot in place, the amputee functions with a more stable, bipedal gait.
For the surgeon to inspect the wound, the prosthetist does not have to be present. The surgeon simply unfastens the Velcro straps and removes the anterior shell of the cast. Instructing the patient to raise the extremity off of the bed by flexing at the hip, the posterior half of the cast can be removed. The Spandex cast socks are removed followed by the dressing. Make note that when reapplying the IPOP cast, the thickness of the gauze dressing must be maintained. The tendency is to apply a lighter dressing, which is counter-productive to maintaining distal compression. The fit of the IPOP cast must be continually monitored. By approximately postoperative day, the residual limb may experience a loss of edema and the IPOP cast becomes loose. An additional Spandex cast sock is applied to improve the fit of the cast and promote further shrinkage of the residual limb. Cast socks continue to be added throughout the time the cast is in place. A sock covering only the distal end of the limb is often used when distal shrinkage is not consistent with the thigh.
On the average, sutures are removed 21–28 days postop- eratively. After suture removal, a total contact below-the- knee prosthesis is fabricated to allow full weight bearing. If possible, the IPOP continues to be used until the total contact below the knee prosthesis is fitted, thereby maintaining func- tion and protection.
CONCLUSION
For the past 7 years, the removable IPOP has proven to be an effective adaptation to the original IPOP concept. The initial goal of the design was to meet the needs of the surgeon, which was to allow for easy wound inspection. The design later proved to be beneficial in the area of physical therapy to allow for strengthening and range of motion. In addition, the prosthetist is aided by the ability to adjust for residual limb volume loss and assist in limb shaping. All lead to a more cohesive clinical team approach with a better understanding of the challenges of postoperative management.
1. Dederich R. Amputationen der unteren Extremitat. Operation- stechnik und prothetische Sofortversorgung. Stuttgart, Thieme, 1970.
2. Berlemont M. Notre experience de l’appareillage precoce des amputes des membres inferieurs aux establissments Helio- Marins de Berck. Ann Med Phys. 1961;4:4.
3. Berlemont M, Weber R, Willot JP. Ten years of experience with immediate application of prosthetic devices to amputees of the lower extremities on the operating table. Prosthet Orthot Int. 1969;3:8.
4. Burgess EM. Immediate postsurgical prosthetic fitting: A system of amputee management. Am J Phys Ther. 1971;51:139–143.
5. Moore WS. Below-knee amputation. In: Moore WS, Malone JM, eds. Lower Extremity Amputation. Philadelphia: WB Saunders Company; 1989:118–131.
6. Wu Y, Krick H. Removable Rigid Dressing for Below-knee Am- putees. Clin Prosthet Orthot. 1987;11:33–44.
The Physical Therapy Assistant program at the University of Cincinnati, Clermont gained valuable, hands on experience today at Premiere Physical Therapy and Abilities in Motion.
Carolyn Shisler, who leads the program at UC, Clermont said that this experience gives future physical therapist assistants the opportunity to hear stories and ask questions to recent and veteran amputees. “They are real people and students are able to hear their story and empathize with their life situation. Our students get to see the person and not the diagnosis,” said Shisler.
Caitlin Rausch participates with PT Training
Caitlin Rausch is a student at UC, Claremont and she echoed those feelings. “It’s so different than being in the classroom. There, you don’t get to see patients and hear their backgrounds”.
Students heard an hour long presentation from experts and then broke into smaller groups to see demonstrations and interact with patients. The patients participating in the program had below knee, above knee and bilateral leg amputations. Each had different experiences that informed students and each saw this as an opportunity to invest in the future.
Andy Beardslee is the PT director at Premiere Physical Therapy and he understands the value of these types of experiences. “Many times, new students are apprehensive when meeting with amputees. They may have a fear of saying the wrong thing and this experience gives them a change to get comfortable with real people.”
Jay Estoquia is a resident at Abilities In Motion
Students would be hard pressed to find a better environment for this type of learning as Premier Physical Therapy is the regions leader in working with amputee patients. Their partnership with Abilities In Motion allows a patient to meet with their prosthetist and physical therapist all in same visit.
Shisler summed up the experience this way, “PTAs work in many different areas of physical therapy, Amputees are one facet of the field. It’s important that they are able to work with people and help them reach their full potential.”
Rodney Jones first came to Abilities In Motion in the summer of 2013. A truck driver for several years, Rodney was injured while on the job. After several failed attempts to reset his leg for healing, the decision was made to amputate Rodney’s left leg.
Rodney worked incredibly hard over the past 1.5 years to get to this place in his life. When Rodney started coming to AIM, Rodney also started working with Premier Physical Therapy (AIM’s inhouse PT). By coming in multiple times each week, Rodney has progressed from using a wheelchair, to parallel bars, to a walker, to a cane and finally has reached unassisted walking. The AIM and Premier teams are extremely proud of Rodney’s progress.
Rodney’s work-related injury forced him to live a very sedentary lifestyle before his amputation.
Though it took a good attitude and a lot of effort, Rodney is now 196 pounds lighter and living the life that he wants to live.
Recently, Rodney started driving by himself again. He has loved being able to regain the independence that he has lacked for so long. Along with AIM’s prosthetic care services and Premier’s physical therapy services, Rodney’s positive attitude has helped him come this far. To him, the amputation was just a “little speed bump” and he finds it important to have fun even in the midst of challenging times. Whether he is driving himself to the hardware store or riding his bike around the neighborhood, it is evident that Rodney is moving forward.
Rodney’s Hardware
As a part of the rehabilitation process, Rodney initially used a prosthesis with a locking knee for 12 months. He then transitioned into using the technologically advanced Orion2 knee from Endolite.
This microprocessor controlled knee unit uses Motion Integrated Intelligence (Mi2), which allows Rodney to feel more secure ashe stands, rides his bike, and walks. This knee can lock at various angles and features progressive speed control. Also,the sensors within the knee allow for Rodney to walk up ramps and hills with more security.
These components have allowed Rodney to progress from initially using a walker to now walking unassisted at variable walking speeds and negotiating ramps and stairs.
Below is our panel of patients, we asked a set of questions concerning their expectations and experiences of surgery, being fit with a prosthesis and learning to walk.
Larry Robinson, 51 is a below knee amputee who had surgery in July of thisyear. Larry had elective surgery with the intent of having less pain and increased activity. He had a target of four weeks to be up and walking, and now believes he will be more active than he first thought. He was walking unassisted in just two weeks!
Larry experiences less phantom pain as time goes by and now has some discomfort but no pain. He quickly adapted to his prosthesis and has mastered sock fit with ease. He cites comfort as his favorite part of his prosthesis and would like to get more flexibility from his ankle to aid with his outdoor lifestyle of fishing and hunting. Larry also mentioned that he would like to have a prosthesis that lets his leg stay cooler.
Walter Lickliter, 57 had a right below knee amputation in July of 2004. Walter also has a left partial foot amputation. His main goal before surgery was to improve his balance and begin the process of learning to walk again. Within two weeks of being fit with his prosthesis, Walter said “I am encouraged by my progress from wheel chair to walker. I have not had any pain since just after the surgery”. He learned quickly through experimentation how to use socks to obtain a correct fit and does not feel his prosthesis limits him. “I like the comfort of my prosthesis and just being able to walk again”.
Tony Freeman, 50 is an above knee amputee who was fit with his first prosthesis in 1999. He said that after surgery the pain was “excruciating, but now I just have phantom pain that is annoying”. He expected to walk with a cane but after his initial fitting he thought he would have to work harder to be able to walk. Later during rehab, his target was to “just walk as normally as possible”. On the subject of learning the correct fit, “I just let my pain tell me what to do”.
“The thing I like most is my mobility, just being able to walk, although I would like to be able to go up stairs step over step”. Since rehab, Tony now cycles regularly and is able to run. Tony also said he would like a more flexible ankle, some rotation and a lighter prosthesis.
Sarah Ammons underwent surgery for a below knee amputation in 2002. Sarah said “I expected to have less pain, as I have a great deal of phantom pain”. She did not expect to be walking unassisted immediately, “I expected a long rehab”. Although undergoing a second surgery earlier this year, she is walking without assistance.
“I am still learning to get the correct fit with socks” says Sarah. I would like to be able to walk longer distances without pain and to be able to go into the ocean. Also as a keen gardener, I would like more flexibility on uneven ground”. She also wanted it to be cooler and lighter.
Sam Crosby has a left below knee and a right partial foot amputation. For Sam, a former college quarterback, rehab went very smoothly. “I just expected to be able to walk and I pretty much did. I knew I would be able to walk without crutches”. Sam reported that he never really had any pain and that learning sock fit was easy.
Sam is active, he plays golf and bowls. “I can pretty much do anything I want to”. “My favorite part of my prosthesis is the air pump that acts like a shock absorber”. Some of the improvements Sam wanted to see were a leg for swimming and a machine washable suspension sleeve.
David Fischer became an above knee amputee just a few months ago in May. David says he wasn’t really sure what his expectations were prior to surgery as it happened so quickly. He said of his expectations upon receiving his prosthesis “I didn’t expect I would just get up and walk. I had a pretty good idea about the rehab process”. After initial fitting and physical therapy, David says he was more confident of being able to return to normal mobility. He has suffered from some phantom pain “but I’m managing well”.
He quickly learned correct sock fit and gave some thought to the question of things he would like to be able to do. “I would like to be able to stand in the shower”. Like many of our panel, being able to walk is one of his favorite things about his prosthesis. As for improvements he would like to see, he agreed with several members of the panel in wanting to be able to get the leg wet and to have a lighter prosthetic foot.
A note from Tom: Thanks to our esteemed panel for their time and thoughtful responses. Hopefully our panel’s shared experiences are relatable to most of you.
These comments will only help us to provide better service. We will also relay this information to our component manufacturers to address the needs of the people we serve.
Some of our panel had some questions for us, so we decided to do a little research.
Here are some statistics you may find interesting.
Approximately 2 million people are living with the absence of a limb in the U.S.
Approximately 40% of amputees are female compared to 60% male.
There are 150,000 amputations every year in the U.S. of which 82,000 people are diabetic.
1 out of every 185 people diagnosed with diabetes undergo amputation of a limb.
The Midwest is the second highest region in the country for amputation. The South is the highest, followed by the Midwest, then the West with the Northeast being the lowest.
There are almost 10 times more below knee amputees than above knee.


 news that his leg would need to be amputated below the knee. Over the past two years he has been partnering with Abilities In Motion to achieve his goals of an active lifestyle.
news that his leg would need to be amputated below the knee. Over the past two years he has been partnering with Abilities In Motion to achieve his goals of an active lifestyle.  During his trip, Brian was able to enjoy the Cliffs of Moher. “I felt comfortable the entire time. My wife was a little concerned that I was standing on a 1,000 foot cliff, but it was easy,” says Brian. He was also able to walk though the Coliseum in Rome and walked for miles on his trip.
During his trip, Brian was able to enjoy the Cliffs of Moher. “I felt comfortable the entire time. My wife was a little concerned that I was standing on a 1,000 foot cliff, but it was easy,” says Brian. He was also able to walk though the Coliseum in Rome and walked for miles on his trip.










 Rodney Jones first came to Abilities In Motion in the summer of 2013. A truck driver for several years, Rodney was injured while on the job. After several failed attempts to reset his leg for healing, the decision was made to amputate Rodney’s left leg.
Rodney Jones first came to Abilities In Motion in the summer of 2013. A truck driver for several years, Rodney was injured while on the job. After several failed attempts to reset his leg for healing, the decision was made to amputate Rodney’s left leg. As a part of the rehabilitation process, Rodney initially used a prosthesis with a locking knee for 12 months. He then transitioned into using the technologically advanced Orion2 knee from Endolite.
As a part of the rehabilitation process, Rodney initially used a prosthesis with a locking knee for 12 months. He then transitioned into using the technologically advanced Orion2 knee from Endolite.

 Walter Lickliter, 57 had a right below knee amputation in July of 2004. Walter also has a left partial foot amputation. His main goal before surgery was to improve his balance and begin the process of learning to walk again. Within two weeks of being fit with his prosthesis, Walter said “I am encouraged by my progress from wheel chair to walker. I have not had any pain since just after the surgery”. He learned quickly through experimentation how to use socks to obtain a correct fit and does not feel his prosthesis limits him. “I like the comfort of my prosthesis and just being able to walk again”.
Walter Lickliter, 57 had a right below knee amputation in July of 2004. Walter also has a left partial foot amputation. His main goal before surgery was to improve his balance and begin the process of learning to walk again. Within two weeks of being fit with his prosthesis, Walter said “I am encouraged by my progress from wheel chair to walker. I have not had any pain since just after the surgery”. He learned quickly through experimentation how to use socks to obtain a correct fit and does not feel his prosthesis limits him. “I like the comfort of my prosthesis and just being able to walk again”.
 Sarah Ammons underwent surgery for a below knee amputation in 2002. Sarah said “I expected to have less pain, as I have a great deal of phantom pain”. She did not expect to be walking unassisted immediately, “I expected a long rehab”. Although undergoing a second surgery earlier this year, she is walking without assistance.
Sarah Ammons underwent surgery for a below knee amputation in 2002. Sarah said “I expected to have less pain, as I have a great deal of phantom pain”. She did not expect to be walking unassisted immediately, “I expected a long rehab”. Although undergoing a second surgery earlier this year, she is walking without assistance. Sam Crosby has a left below knee and a right partial foot amputation. For Sam, a former college quarterback, rehab went very smoothly. “I just expected to be able to walk and I pretty much did. I knew I would be able to walk without crutches”. Sam reported that he never really had any pain and that learning sock fit was easy.
Sam Crosby has a left below knee and a right partial foot amputation. For Sam, a former college quarterback, rehab went very smoothly. “I just expected to be able to walk and I pretty much did. I knew I would be able to walk without crutches”. Sam reported that he never really had any pain and that learning sock fit was easy. David Fischer became an above knee amputee just a few months ago in May. David says he wasn’t really sure what his expectations were prior to surgery as it happened so quickly. He said of his expectations upon receiving his prosthesis “I didn’t expect I would just get up and walk. I had a pretty good idea about the rehab process”. After initial fitting and physical therapy, David says he was more confident of being able to return to normal mobility. He has suffered from some phantom pain “but I’m managing well”.
David Fischer became an above knee amputee just a few months ago in May. David says he wasn’t really sure what his expectations were prior to surgery as it happened so quickly. He said of his expectations upon receiving his prosthesis “I didn’t expect I would just get up and walk. I had a pretty good idea about the rehab process”. After initial fitting and physical therapy, David says he was more confident of being able to return to normal mobility. He has suffered from some phantom pain “but I’m managing well”.